Nerves & Circulation
PLEASE NOTE: We are not medical professionals, and the information on this page should not be considered medical advice! What we present here is the best information we have at this time based on our research and consultation with others who do have medical training. Use this information at your own risk, and remember that all rope bondage is dangerous and carries the risk of injury. You should research this information for yourself. We also highly recommend First Aid and CPR training for all rope practitioners. In nearly all cases below, if you are medically trained, you will have more informed options that you may choose to pursue beyond the ones listed here. These steps are intended to help those without medical training to provide assistance while also not causing further harm. Finally, if you are injured, our best advice is to seek medical treatment from a qualified facility.
Circulation Loss vs. Nerve Compression
Circulation Loss
Generally speaking, circulation loss over a short period of time isn’t a major concern, and neither is the discoloration that typically accompanies it. In fact, discoloration is a particularly unhelpful guide for assessing risk because of the extreme variability among people: some discolor quickly and drastically, others show little to no change regardless of the degree or time involved in circulation loss.
That being said, the skin becoming darker (purple or red-ish) typically indicates impaired venous return, which is common in rope bondage and generally not a concern over short periods of time (30 minutes or so).[note]See “Purple limbs and rope bondage- when should you worry?“[/note] However, the skin becoming paler can indicate impaired arterial flow, and this is a much more serious condition which should be immediately addressed. Thankfully, impaired arterial flow is difficult to achieve because arteries tend to be buried more deeply in the body and therefore are more difficult to compress. [note]For a more thorough discuss on Remedial Ropes: Circulation[/note]
In emergencies, a limb can be without circulation up to 2 hours without negative long-term effects and between 30 to 45 minutes with no changes to the muscles at all; however, the general rule of thumb for first-aid tourniquets is 1 hour for upper-extremities and 2 hours for lower-extremities. (However, note that individuals with pre-existing circulation issues — such as Raynaud’s syndrome, peripheral vascular disease, diabetes, etc. — are at greater risk.) [note]Reference 1 – Reference 2 – Reference 3[/note]
In the bondage world, most people will err on the side of safety and not allow blood flow to remain restricted for more than 15 to 20 minutes and will also take steps to improve circulation by dressing or moving wraps, changing positions, etc. Of course, in some cases, circulation loss is unavoidable (such as a single-leg suspension, for example).
That said, it should be noted that circulation loss can occur simultaneously with nerve impingement, and in some cases, circulation loss can contribute to nerve impingement. However, the larger concern with reduced circulation is that it can mask damage to the nerves. For example, loss of sensation could be due to loss of blood flow … or it could be the result of a compressed nerve. Therefore, it’s important to realize that when circulation is reduced, the risk of missing other important warning signs is increased, and the most common type of injury in that situation is nerve damage.
Nerve Compression
Nerve damage is the most insidious danger of rope bondage. It can happen instantly or gradually over multiple scenes. It can be masked by circulation problems. It can heal in an hour or a month or a year … or never.
Therefore, it’s important that both tops and bottoms recognize that this risk is always present, and while sometimes injury may occur due to “fault” on someone’s part, it may also occur as an unavoidable outcome of this type of activity—for which no one is to blame.
Our best advice is for tops and bottoms to learn as much as they can about the types of nerve injuries possible during rope bondage and how best to mitigate the risks, recognize the symptoms, and respond to injuries should they occur. It’s also important that bottoms learn as much as they can about their bodies in order to help tops tie them in ways that are most appropriate for the bottoms’ specific needs.
Once a bottom indicates that they’re experiencing numbness due to circulation, the burden shifts to the top to closely monitor for signs of nerve compression. And if the bottom allows the tie to continue to the point of one or more limbs going completely numb, the top must monitor closely and continually. In those situations, the bottom should recognize the additional risks they are taking.
Nerve Functioning & Common Indicators
The nerves in your body serve one or both of the following functions:
- Provide sensation (referred to as “innervation”) to a particular part of the body
- Provide motor functions (referred to as “mobility”) to a particular part of the body
When nerves are compressed or otherwise damaged in some way, the following symptoms typically occur (though not always and not always immediately):[note]”Stop Getting On My Nerves! Nerve anatomy for rope bondage.” MissDoctor[/note]
- tingling or burning sensation
- numbness or loss of sensation
- weakness or loss of mobility
Though many people report that these symptoms tend to occur in that order, one or more symptoms may occur at the same time. It’s also possible that no warning symptom will present until after damage is done.
Common Causes & Contributing Factors
There seem to be three common causes of nerve injury that relate to rope bondage:
- Direct mechanical stress on the nerves: meaning that the rope is on or very near to the nerve, and the pressure of the rope causes stress or compression to the nerve, resulting in injury
- Indirect stress on the nerves: meaning that the pressure of the rope and/or the positioning of the body causes stress or compression to the nerve indirectly (which can happen even when the rope isn’t positioned over the nerve) resulting in injury; this can result from ties that cause a great deal of stretching, torsion, and similar kinds of physical stress
- Anoxia/ischemia of the nerves: meaning that the oxygen and blood supply to the nerve is restricted and causes slowing or cessation of both sensory and motor nerve function
There are also a few common indicators associated with an increased chance of nerve compression injury, including: history of smoking, diabetes, familial neuropathies, alcoholism, and anatomic anomalies.
Another potential factor is the “Double-Crush Symptom,” which theorizes that nerve compression at one site can cause an increased chance for compression injury at another site. [note]Mackinnon, Susan E. & Christine B. Novak “Compression Neuropaties” Green’s Operative Hand Surgery 28, 921-958, 2017. Electronic.[/note] To be safe, if addressing the immediate, suspected area of concern doesn’t have a positive effect, remove all rope along the system (or, if unsure what that system is, remove all rope).
It’s also worth noting here that people with “loose” skin (elderly, someone who experienced recent, drastic weight-loss, etc.) or people with large amounts of subcutaneous tissue (typically comprised mainly of fat cells) may be at greater risk of experiencing nerve injury through the shearing forces that usually occur at the edge of a cuff or band of rope. This is because the rope will hold to the skin, but the skin itself may allow the rope and the skin to rotate back and forth, causing shearing, which can injure the nerve. In these cases, take extra precautions to make sure the cuff is tensioned evenly, to make sure the cuff is tensioned correctly to fit the shape of the body part being tied, and to make sure the band is wide enough to appropriately distribute the load it will take.
One other contributing factor to the likelihood of nerve compression injury is physical variability: some people are simply more prone to nerve compression injury than others. Palpating common vulnerable nerves and noting both sensitivity and location can help reduce risk. In addition, certain types of diseases (such as multiple sclerosis (MS) and other demyelinating diseases) can make people more vulnerable to nerve compression injuries.
Prevention through “Tying Well”
Throughout this course, we will try to provide specific recommendations, exercises, and tips to help tops “tie well,” to help bottoms recognize when something is or isn’t being tied well, and to help both communicate effectively. However, the following general guidelines relate directly to mitigating risk of nerve injury:
- The more vulnerable the location, the greater the risk. Certain nerves are more vulnerable in some anatomical locations than in others. Learning the general areas of vulnerability and tying in ways that avoid or minimize compression in those areas is an important first step. Learning about the specific vulnerabilities of the person(s) you are tying is an essential second step. Putting these two things in the context of the other issues discussed on this page is a necessary third step.
- The longer the rope is on the body, the greater the risk. One implication is that “more intense” or “more risky” rope should be shorter in duration. Another implication is that the top’s control and efficiency are an important safety factor.
- The greater the tension of the rope, the greater the risk. Tension should always be “sufficiently tight” but not tighter. What constitutes “sufficiently tight” will vary depending on the tie, the purpose of the tie, and the body being tied; however, in general, you want the minimal tension required to prevent the rope from moving, shifting, or changing tension throughout the scene. This is also why partial suspension work typically involves greater risk than floor work and why full suspension work typically involves the greatest amount of risk.
- The more narrow the band, the greater the risk. A wider band can distribute the pressure across that band more evenly (assuming even tension in the band), thereby reducing the risk of injury.
- The more uneven the tension in the band, the greater the risk. If one wrap or one line in a band of rope is tighter than the others, the body will primarily suffer the stress of that tighter wrap or line. In other words, if one line in a cuff is noticeably tighter than all the others, the cuff acts as if it consisted of only that single line (which returns us to “the more narrow the band …”). Also, if the rope is twisted or if lines or bands overlap, that will cause greater tension and pressure at the site of the overlap or twist, leading to the same effect.
When we combine these concepts with the common causes above, it becomes clear that merely “putting the rope in the right place” or “avoiding putting the rope in the wrong place” is only one part of mitigating the risk of nerve injury. Therefore, as helpful as diagrams like the ones below may be, they are not all we need to consider when thinking about preventing nerve injury.
Repetitive Injury
It’s also worth noting here that repetitive injury, to one degree or another, seems to be fairly common among experienced rope bottoms. This means that the nerve (and usually the same nerve or group of nerves, typically related to the same tie and similar placement) is stressed incrementally over many different rope sessions — none of which are severe enough to cause noticeable injury individually. However, over time, those micro-injuries can add up until a particular rope session causes the injury to become apparent.
This can happen even if the rope is “tied well” each time. Remember, the type of rope bondage we practice is inherently dangerous and injury (including micro-injury) happens even to experienced bottoms being tied well by experienced tops.
In that case, it’s important to note that this latest rope session may not have “caused” the injury by itself, and so the top during that session isn’t “to blame” (provided the top was tying well, good communication happened, and other precautions were taken). This is simply one of the risks of rope bondage that both tops and bottoms should understand in order to practice rope in a risk-aware manner.
Some “False Negative” Tests
There are a number of indicators and checks that both tops and bottoms can do to help them distinguish between circulation loss and nerve compression. However, we call these “false negative” tests because it’s possible to “pass” them and still end up with some type of nerve damage. Still, they’re the best we have, and are worth doing regularly.
| Circulation Loss | Nerve Compression | |
| Speed of Sensation Loss | Gradual | Sudden |
| Area of Sensation Loss | Whole Limb | Partial Limb / Fingers |
| Mobility Checks | No Loss of Mobility | Loss of Mobility |
| Capillary Nail Refill | Slow Refill | Normal Refill |
- Speed of the Sensation Loss: Loss of sensation due to circulation loss appears gradually, and usually in stages (slight tingling, fat fingers, more intense pain, complete numbness … the specific sensations and steps may vary from person to person). Loss of sensation due to nerve compression could be gradual or sudden. Therefore, sudden sensation loss warrants immediate attention, but gradual sensation loss doesn’t necessarily mean you can attribute it to circulation.
- Area of Sensation Loss: Loss of sensation due to circulation tends to affect the entire limb or hand/foot. Loss of sensation due to nerve compression tends to affect only a portion of the hand or foot (see below).
- Mobility Checks: (establish a baseline before tying) The inability to move the hands or feet in particular ways can indicate nerve compression. See below for details.
- Capillary Nail Refill: (establish a baseline before tying) Press on the nail of a finger or toe until it turns white. Release, and see how quickly color returns to the nail. If it takes longer than a second or two, circulation loss is likely.
Major Areas to Watch

Most rope practitioners are warned early on to avoid tying tightly around joints. Not only are joints weaker areas of the body, but nerves are typically exposed in these areas, so compression is more likely. In addition, the general advice to tie on the meaty parts of the limb or body is also helpful, as muscles tend to protect the nerves. However, this advice has more nuance: it is not always true at every location, and in some instances, muscles can contribute to the compression. Therefore, in addition to this general advice, we recommend that you familiarize yourself with the nerves listed below, their vulnerable locations, and the implications of compressing them.
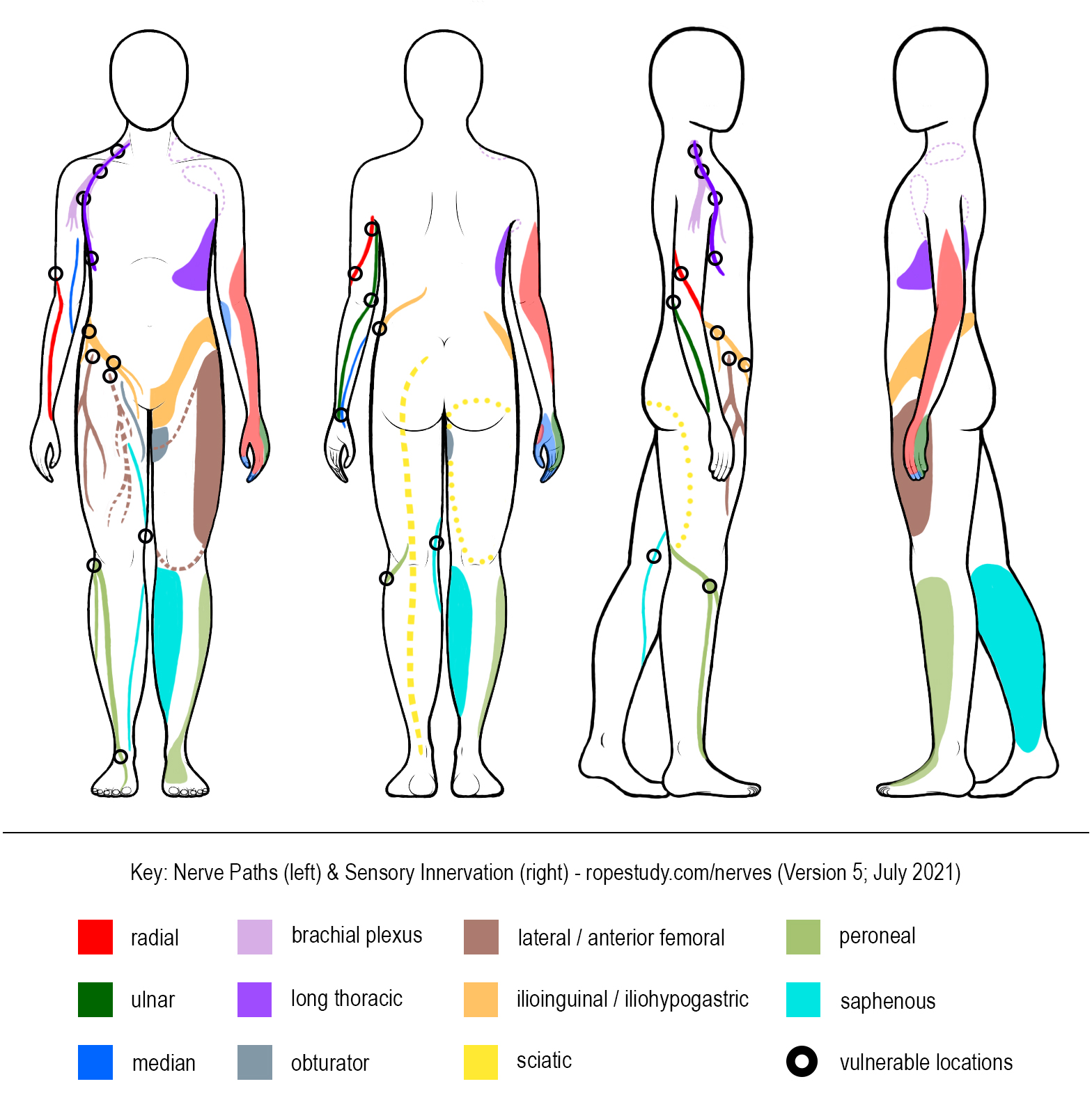
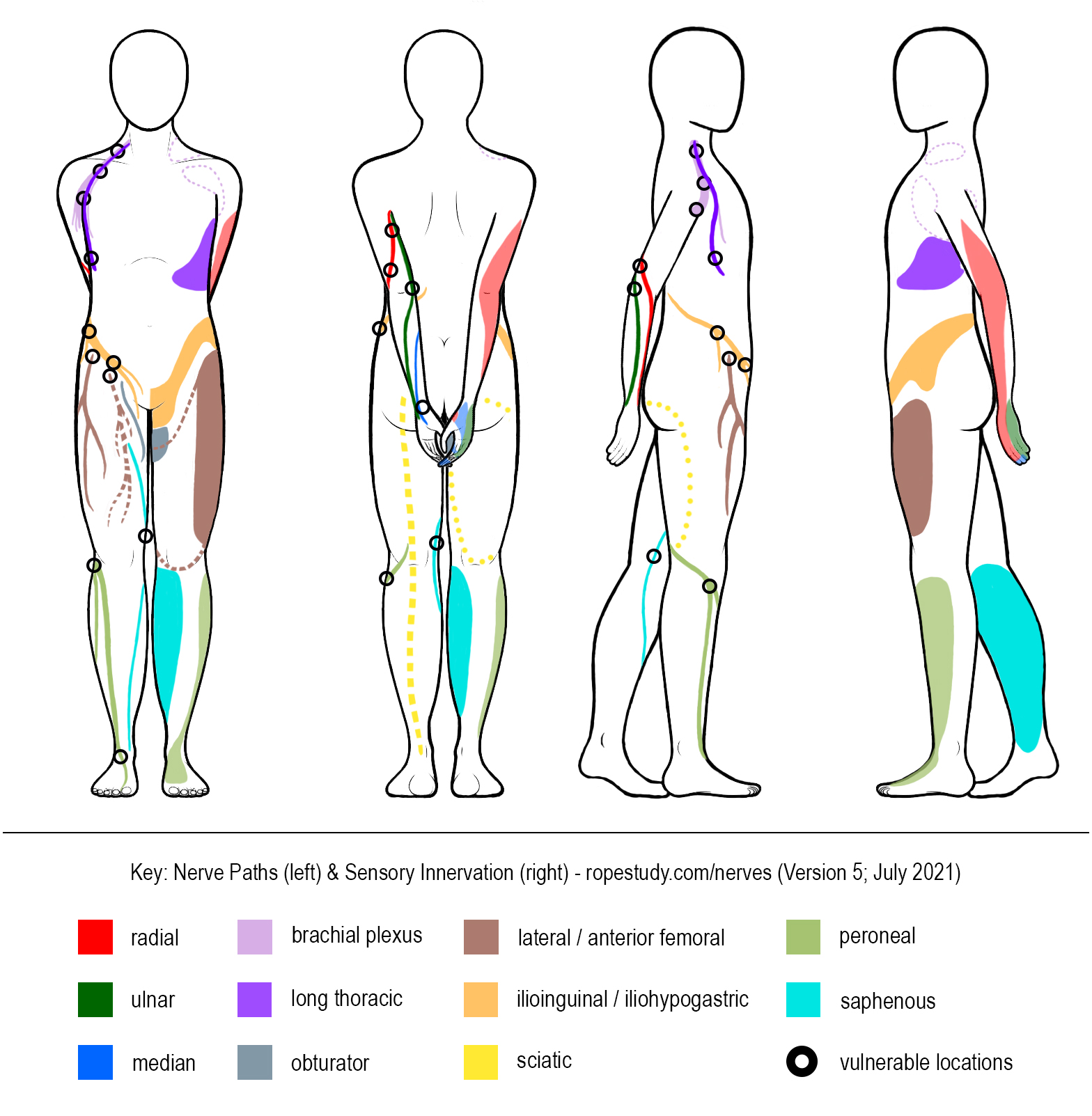
The diagrams below should give you a general sense of the path and sensory innervation for these nerves. However, please note that we provide these only as general reference! Statistically, for around 80-85% of people, the location of any given nerve will roughly line up with the diagram below, but that means that this diagram is not accurate for 15-20% of people (roughly 1 in 5) for any given nerve (not to mention that this diagram is not drawn to scale)! This diagram is a helpful general reference, but each body is unique, and spending time learning about the particular concerns of each body in rope is time well spent.
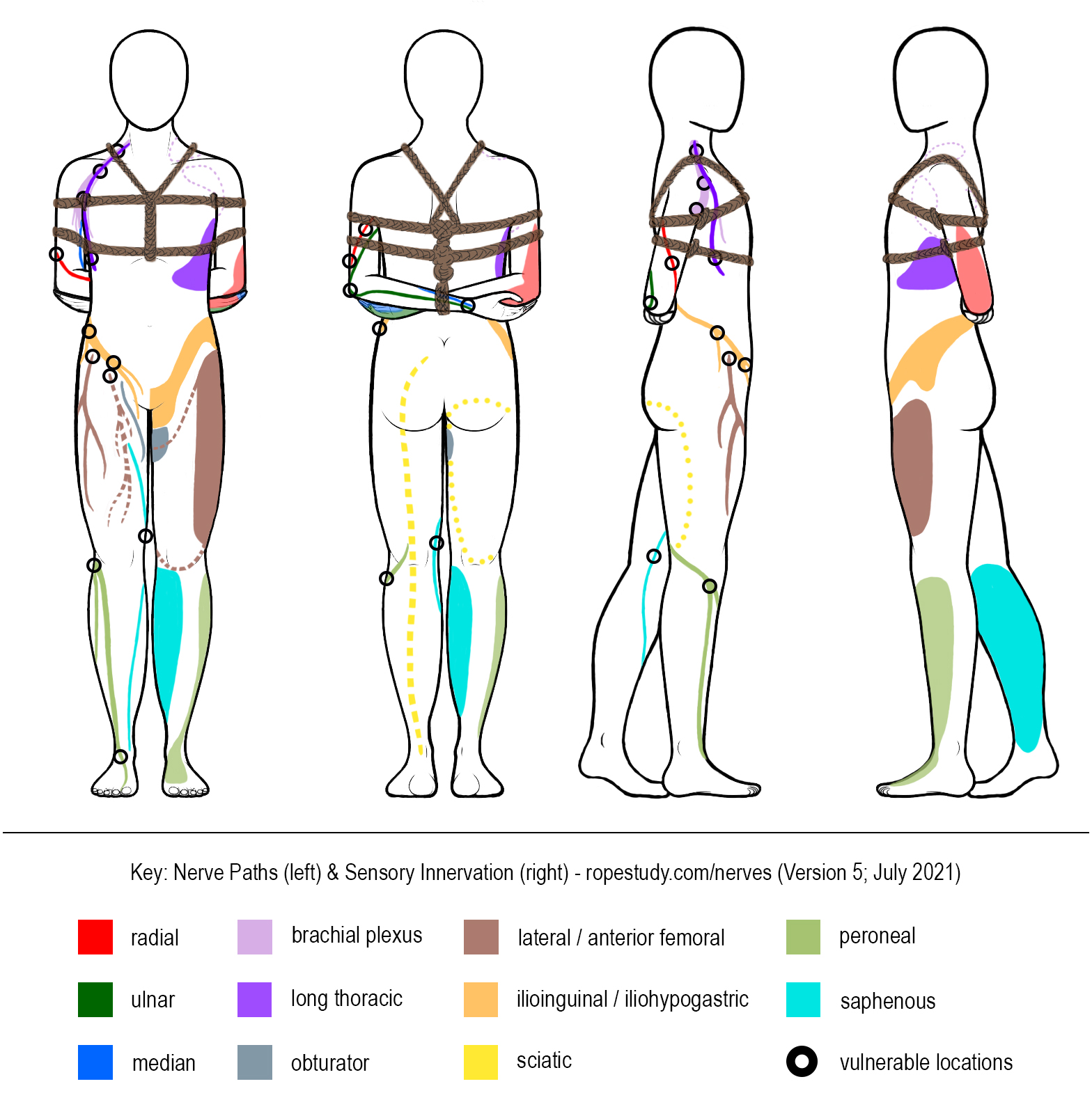
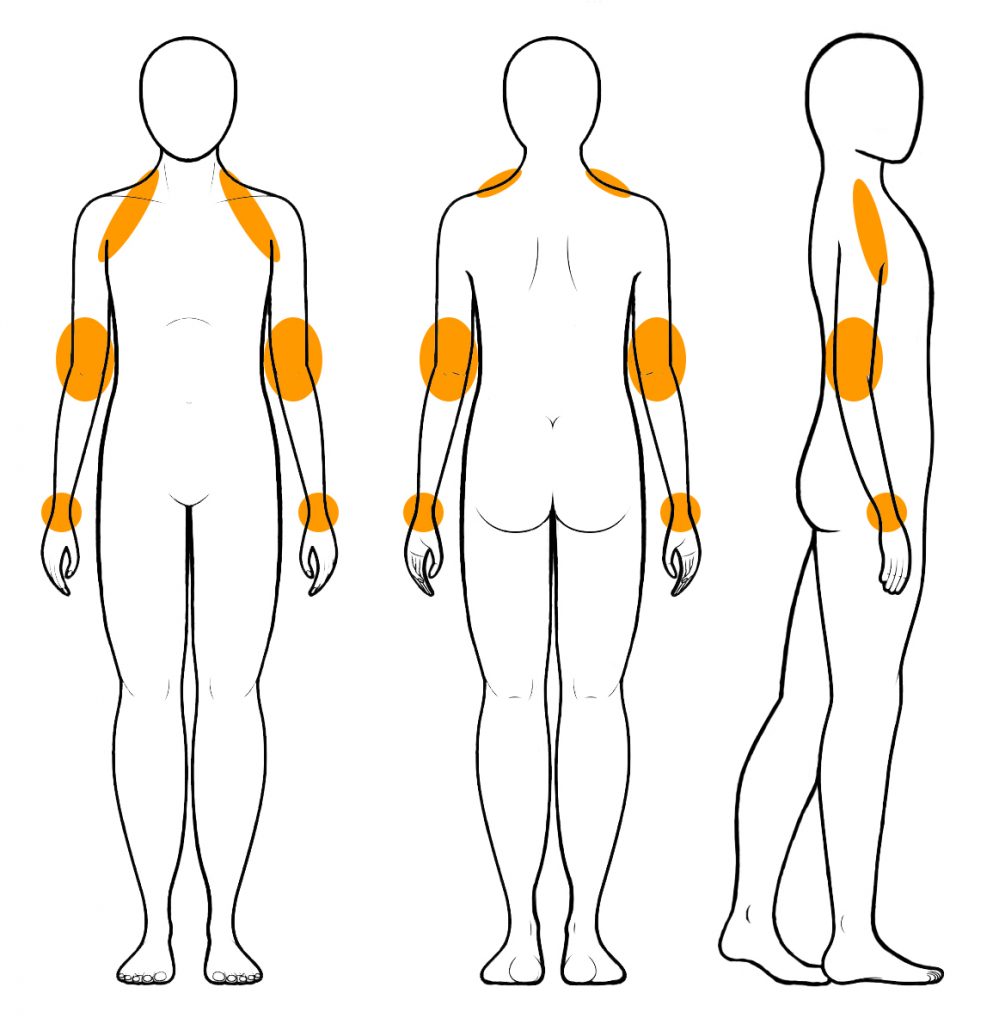
A Closer Look at the Arm: Locations, Indications, and Implications
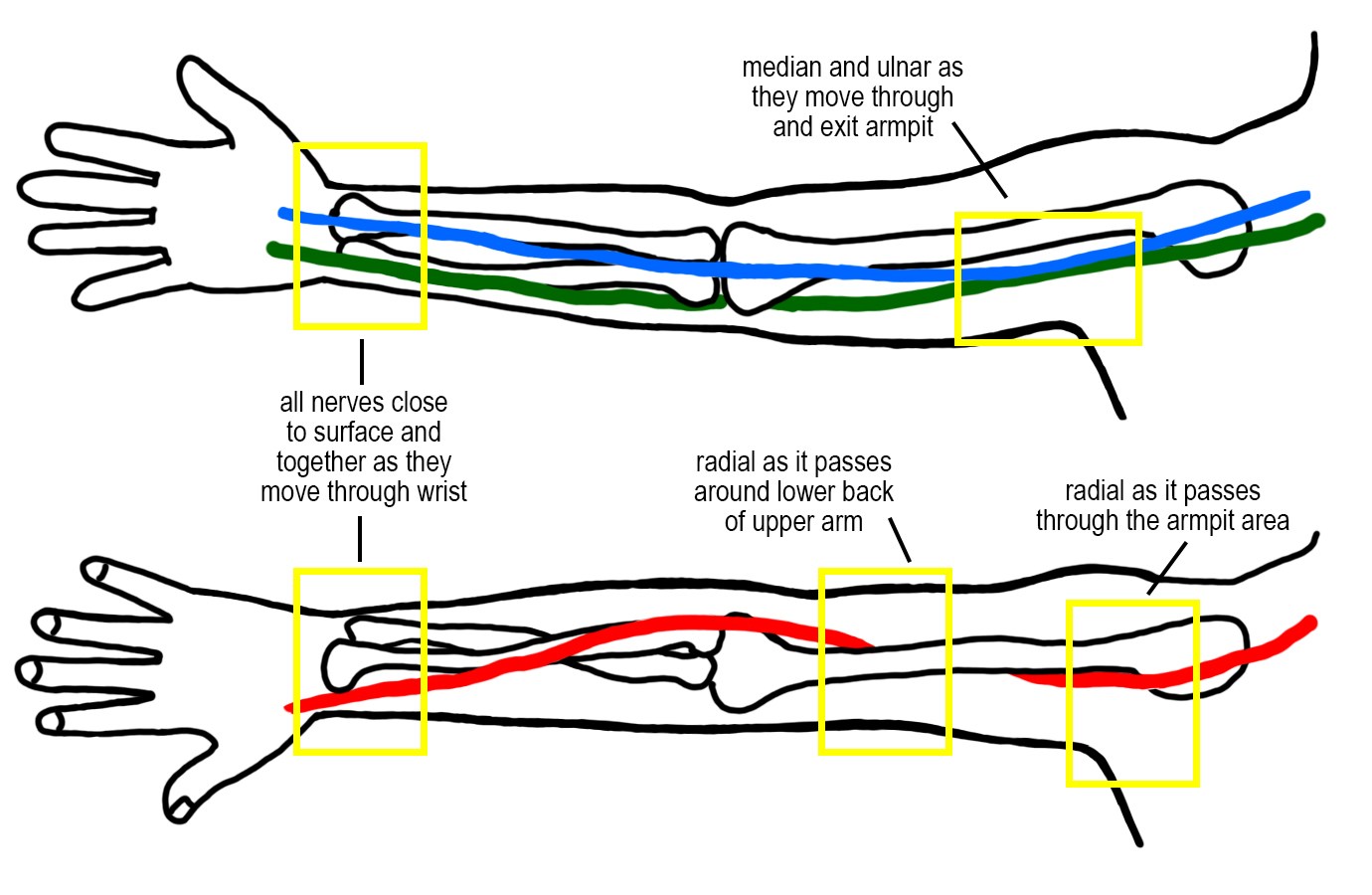
Many nerve-related injuries affect the arms, so let’s take a closer look and point out a few particularly problematic areas: the armpit region, the lower region of the upper arm, and the wrist.
Major Nerves to Consider
- Brachial Plexus (Note: even though the brachial plexus is technically in the neck and shoulder region, compression often results in symptoms that exhibit in the arm, which is why we include it here.)
- More-Vulnerable Locations: As it exits the neck, branches at the front of the chest (the “dip” near the corner of the neck and shoulders), and runs through / under the armpit.
- Rope Placement: Passing rope over or under those areas can cause compression, in particular: shoulder bands on ties with knots near the front of the neck or thin bands that are loaded too close to the neck; rope wedged into the armpit (thick rope or knots in this area are more likely to cause compression) [note]See “The Brachial Plexus – Animated Review” and “The Brachial Plexus II: Animated Review“[/note]
- Results of Compression: This can be tricky as compression of the brachial plexus can (and often does) present as compression of the radial, ulnar, or median nerve.
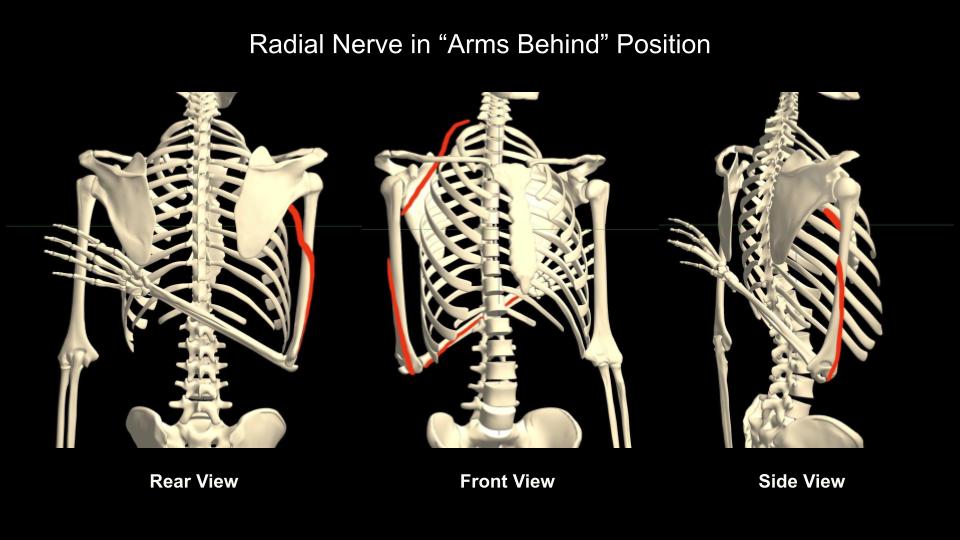
- Radial Nerve
- More-Vulnerable Locations: The radial tends to pass around the back of the upper arm to the forearm at or just below the midway mark of the upper arm, and is more vulnerable as it exits the brachial plexus under the arms and as it runs around the back of the upper arm to move towards the forearm. The radial can also be compressed around the wrists.
- Rope Placement: This is the nerve most-commonly injured by ties that include rope over the arms; as a result, many advise keeping rope away from the lower half to lower third of the upper arm, particularly along the back of the elbow. [note]Hasan, Syed & B Rauls, Russell & L Cordell, Cari & S Bailey, Mark & Nguyen, Thao. (2014). Zone of Vulnerability for Radial Nerve Injury: Anatomic Study. Journal of surgical orthopaedic advances. 23. 105-10. 10.3113/JSOA.2014.0105.[/note]
- Results of Compression: Symptoms include: loss of sensation along a portion of the back of the hand (middle and index finger and thumb); an inability to hold the hand in line with the arm or to flex the hand and fingers backwards, often referred to as “wrist drop.”
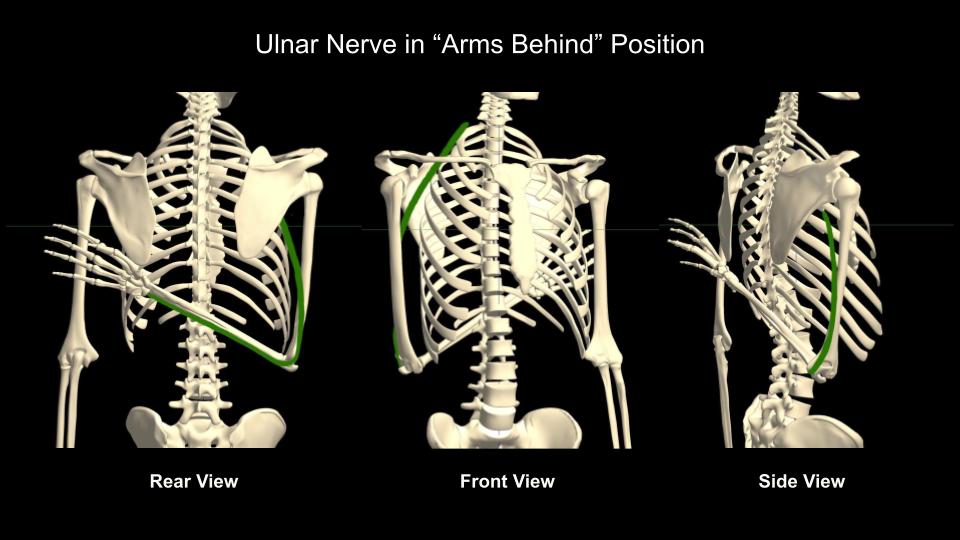
- Ulnar Nerve
- More-Vulnerable Locations: Most vulnerable as it runs behind the elbow, as it moves through the wrist, and as it exits the brachial plexus under the arms.
- Rope Placement: This nerve is most likely to be compressed by tight or loaded rope very close to the elbow or around the wrist.
- Results of Compression: Loss of sensation in the pinky and ring finger; inability to turn/twist the hand in the direction of the pinky.
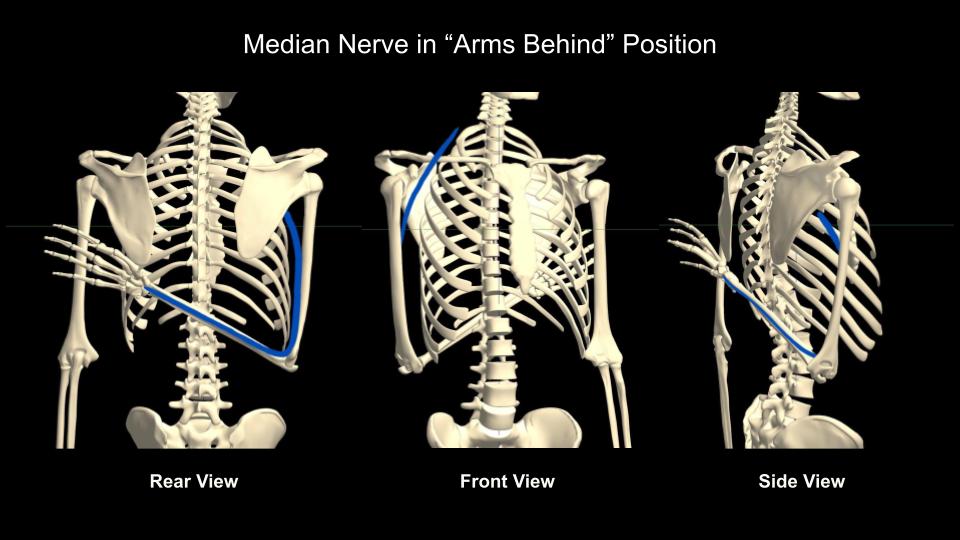
- Median Nerve
- More-Vulnerable Locations: Most vulnerable as it moves through the wrist and as it exits the brachial plexus under the arms.
- Rope Placement: This nerve is most likely to be compressed by tight or loaded rope very close to the wrist.
- Results of Compression: Loss of sensation in the tips of the fingers (index, middle, and ring fingers); inability to make a tight fist.
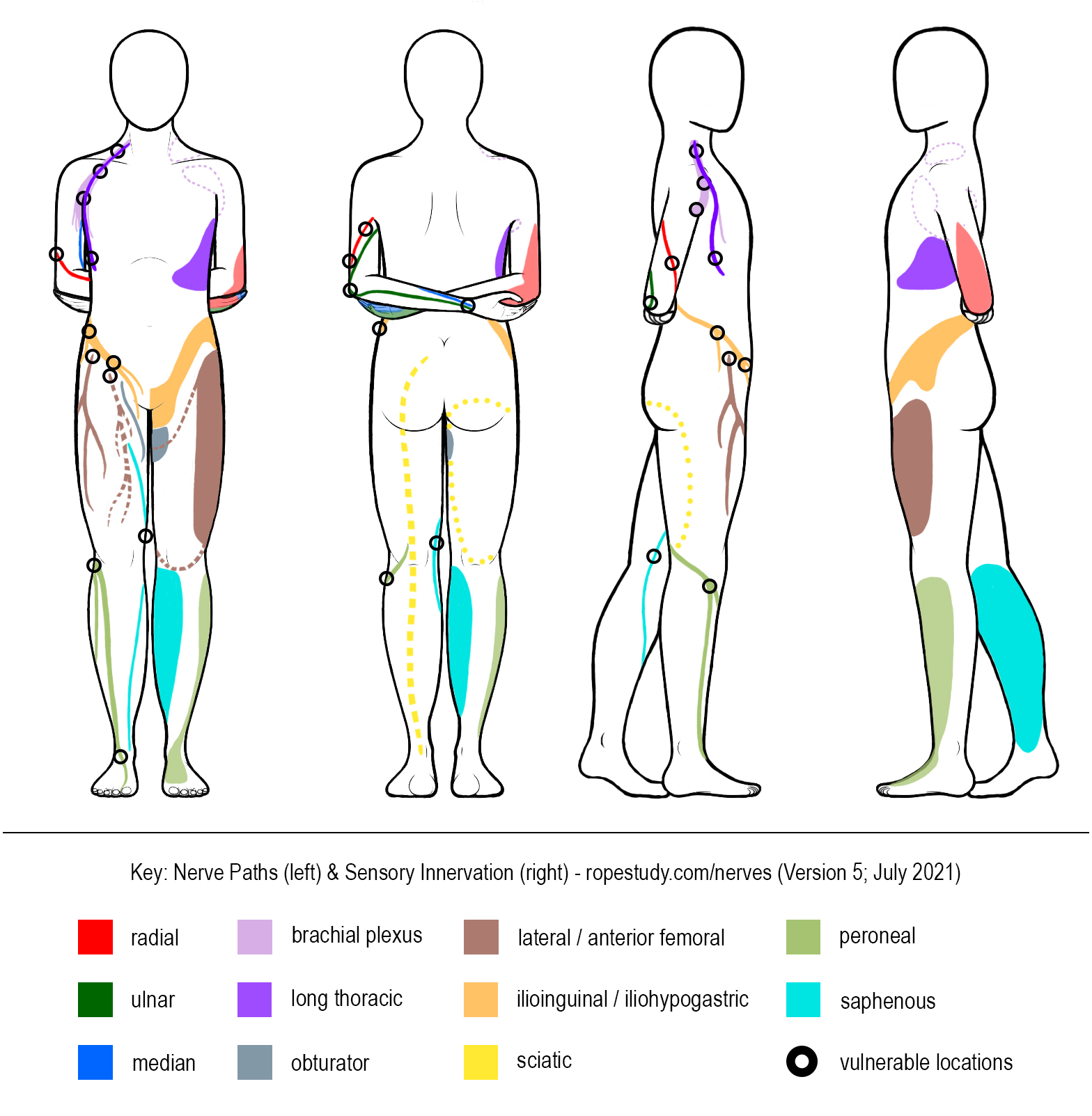
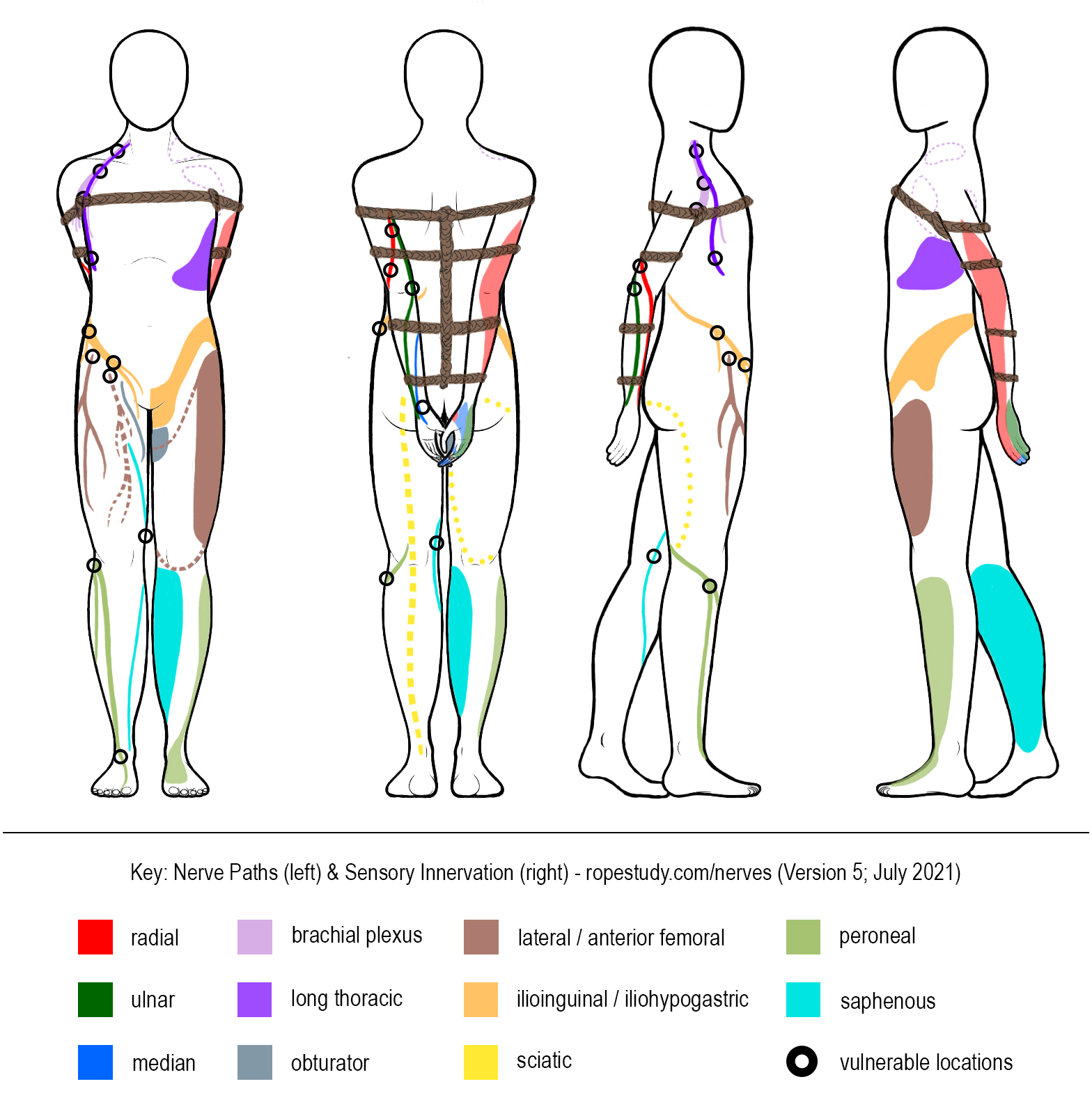
General Nerve Paths in “Arms Behind” Position
Major Indicators
Decreased sensation, numbness, tingling, or a burning sensation in a given area of the hand can indicate possible nerve compression or damage to the corresponding nerve somewhere along the arm (see the diagram below).
In addition, the inability to move the hand in particular ways can indicate a problem with a specific nerve as well:
- Ulnar Nerve – difficulty turning the hand (as if turning a door knob) in the direction of the pinky
- Median Nerve – difficulty bending the hand forward (toward the forearm) or making a tight fist
- Radial Nerve – difficulty flexing the hand backwards or giving a “thumbs up”
Innervation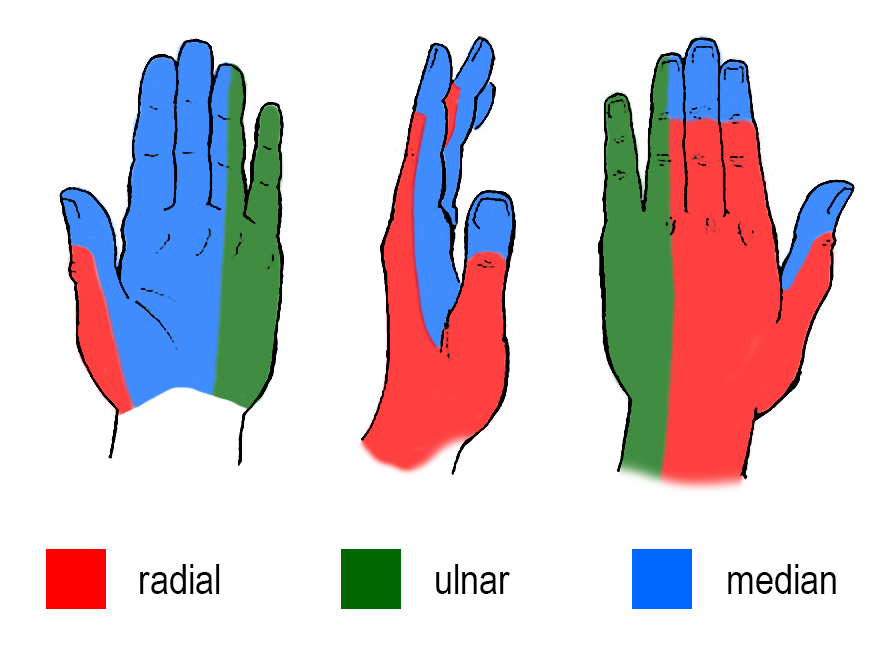
Mobility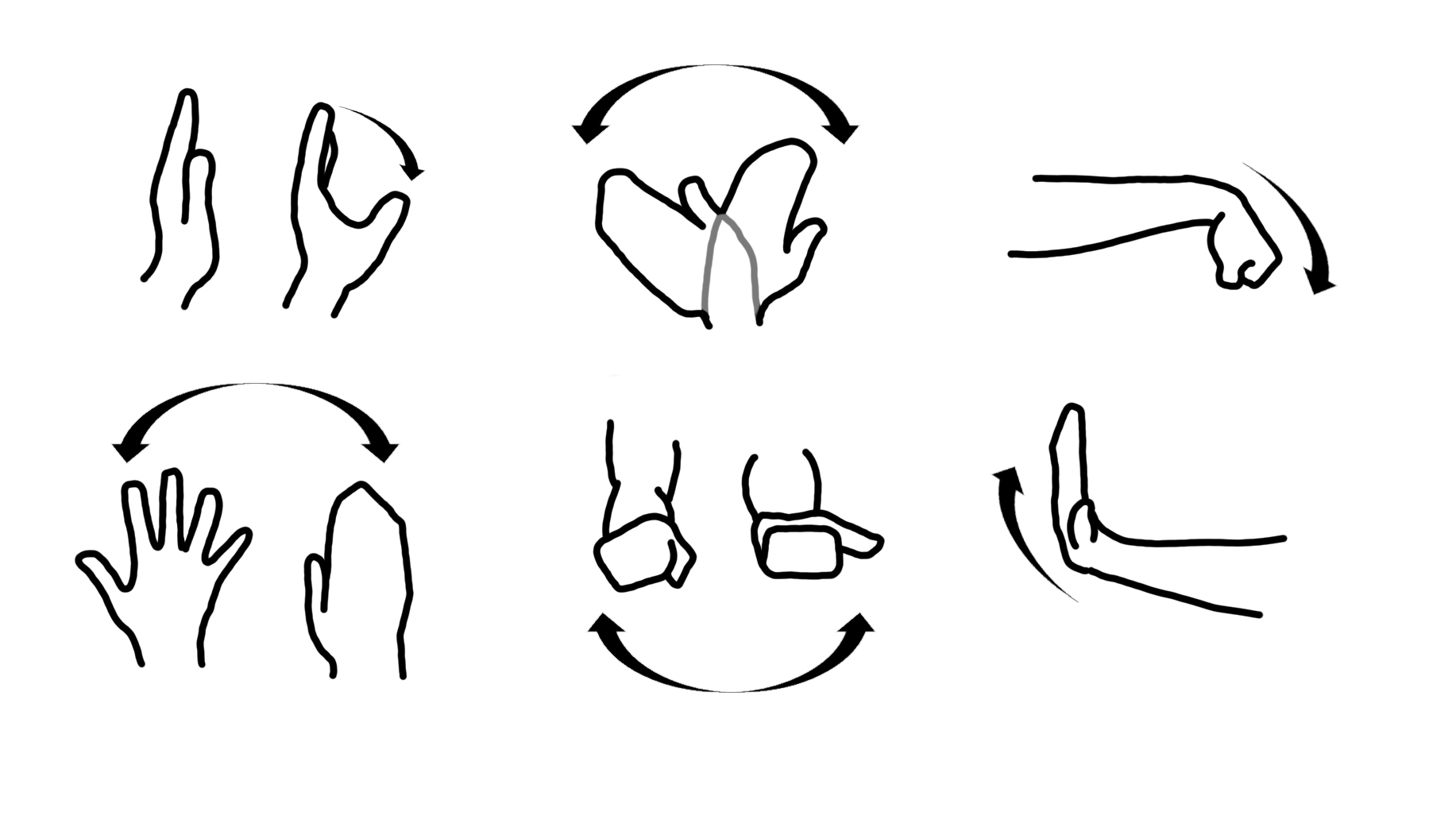
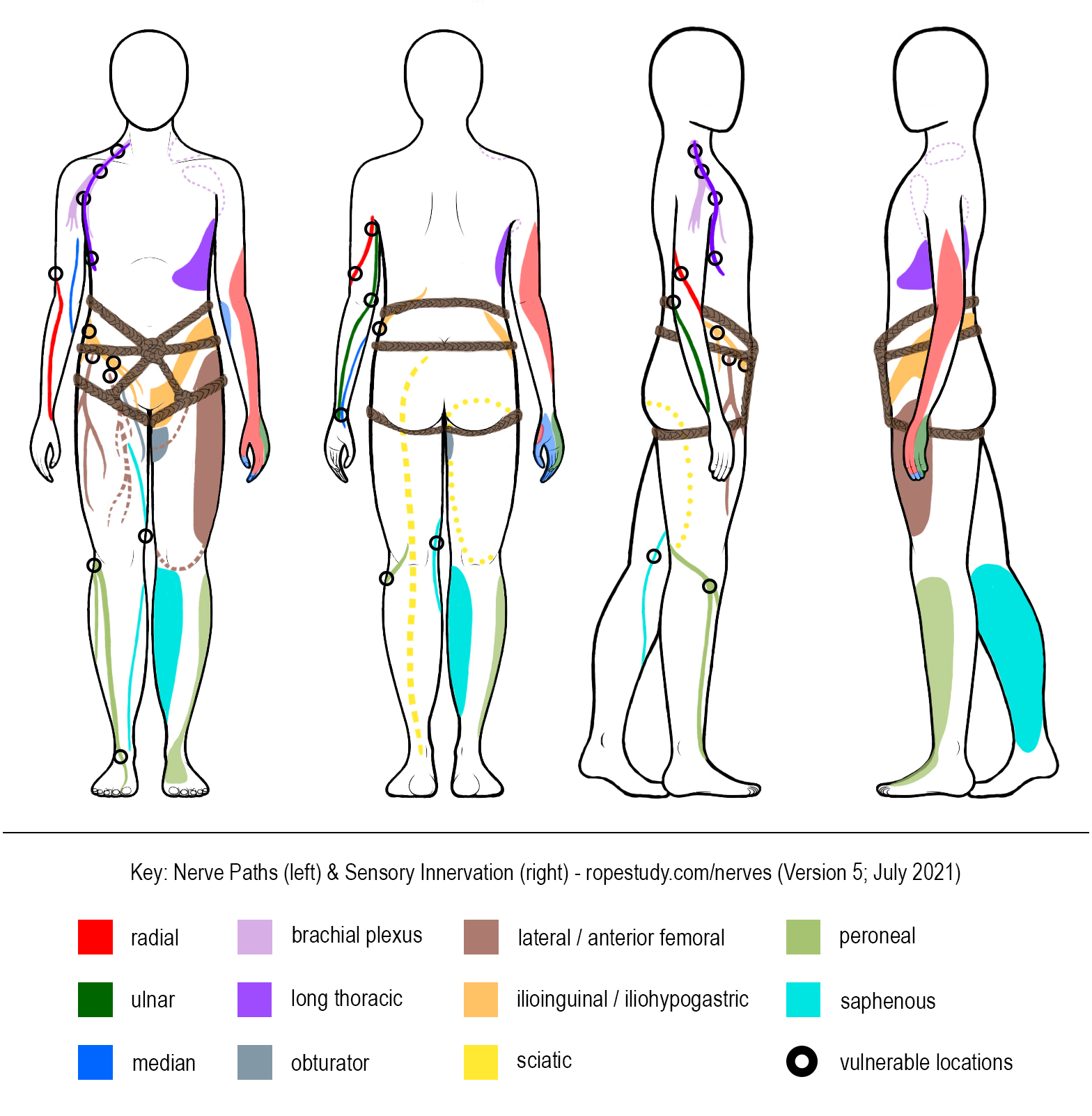
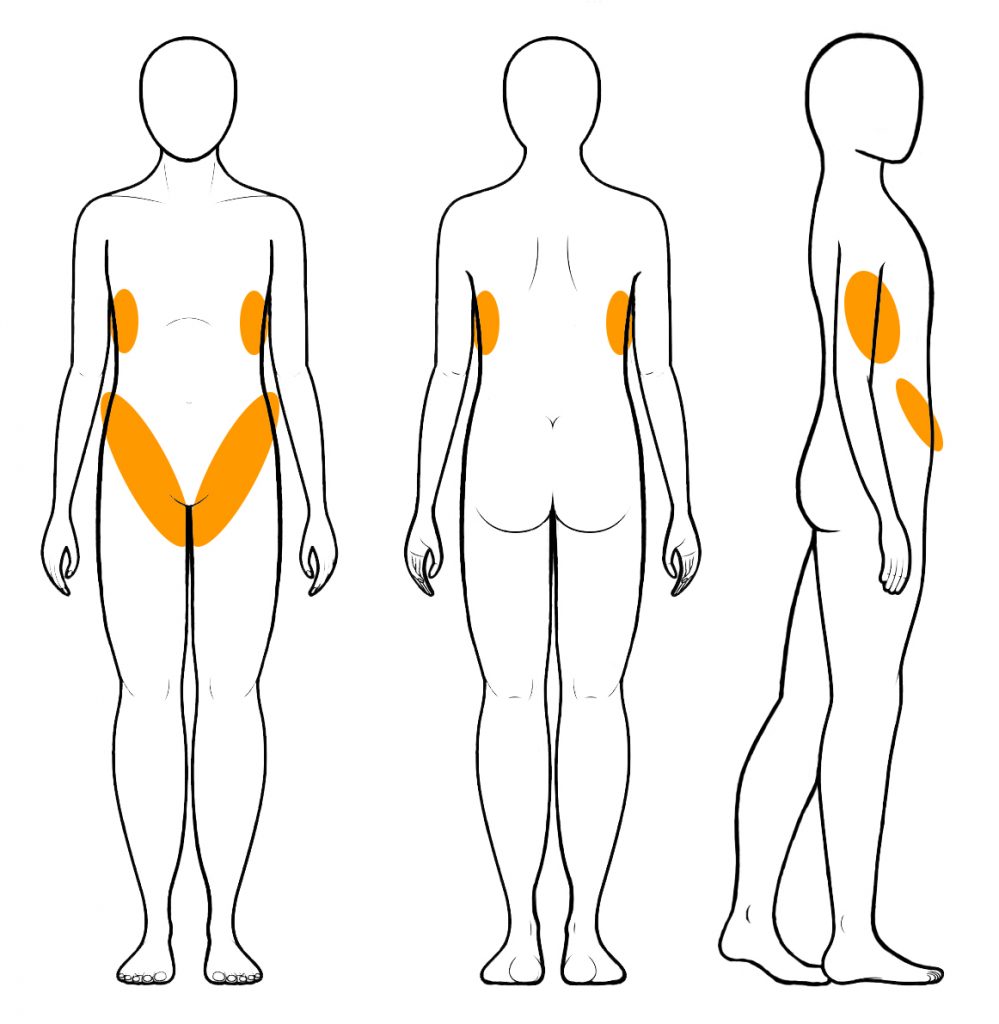
A Closer Look at the Torso: Locations, Indications, and Implications
Compression-related injuries in the torso and hips tend to result mainly in sensation loss rather than limitations in movement, but these can still create challenges to normal movement and functions. The major areas to watch here are along the side of the ribcage, along the top of the hip bones, and along the “panty line” in the crease of the leg and thigh.
Major Nerves to Consider
- Long Thoracic Nerve
- More-Vulnerable Locations: Along the side of the rib cage. This nerve is particularly vulnerable due to extreme flexion (arms tie overhead, for example).
- Rope Placement: Rope that passes tightly across the sides of the rib cage (common in chest harnesses) can contribute to compression, particularly when loaded in suspension and when the upper body is in flexion.
- Results of Compression: Decreased sensation, numbness, tingling, or a burning sensation between the shoulder blades, along the side of the ribs, and moving into the front of the chest below the breast. Can also result in a feeling of tightness in the chest and difficulty breathing. Particularly susceptible to cumulative injury. Over time, this can result in “winging of the scapula” where the shoulder blades jut out at rest (instead of folding along the back). Without correction, this can lead to the shoulders doing extra work to maintain proper positioning, which can then result in complications with the shoulder.
- Lateral Femoral Cutaneous Nerve
- More-Vulnerable Locations: As it runs across the outside and front of the hip and along the crease of the leg and hip. (Note that this positioning is similar to the ilioinguinal and iliohypogastric nerves.)
- Rope Placement: Rope passed over the hips and loaded in face-down suspension is particularly likely to cause compression. This is the nerve most-commonly injured by ties that include rope around the hips. [note]See “Rope Incident Report – Injury to the Lateral Femoral Cutaneous Nerve” for detailed discussion[/note]
- Results of Compression: Decreased sensation, numbness, tingling, or a burning sensation along the top of the thigh or knee, or weakness of the knee or leg when bearing weight (and particularly in movements or positions similar to walking down stairs) could indicate compression of the femoral nerve.
- Ilioinguinal and Iliohypogastric Nerves
- More-Vulnerable Locations: As it runs along the iliac crest (top of hip bone) and along the crease of the leg and hip. (Note that this positioning is similar to the femoral nerve.)
- Rope Placement: Waist and hip rope that is loaded in an inversion is particularly likely to cause compression.
- Results of Compression: Decreased sensation, numbness, tingling, or a burning sensation in the region of the groin could indicate compression of the ilioinguinal or iliohypogastric nerves.
- Obturator Nerve
- More-Vulnerable Locations: As it exits the groin on the inner thigh.
- Rope Placement: Ropes that bind tightly around the upper thigh may cause compression. This seems to be highly variable in both location and sensitivity. This is typically the nerve that causes people to have specific preferences about how high or low into the groin area they prefer upper-thigh rope (such as in a folded-leg tie).
- Results of Compression: May cause tightness or burning when the rope is loaded and may result in loss of sensation or tingling near the groin on the inner part of the thigh.
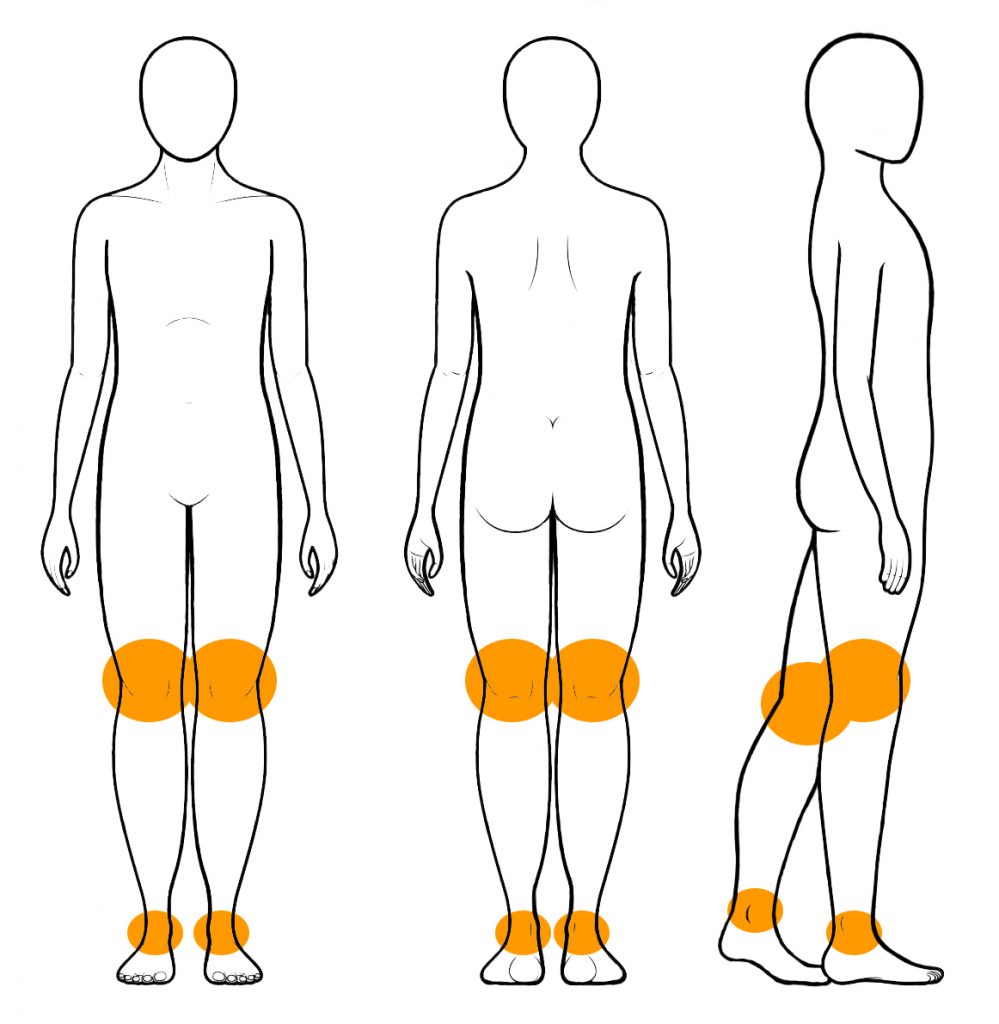
A Closer Look at the Leg: Locations, Indications, and Implications
The major areas to consider in the leg are around the knee and ankle. Avoid tight rope around either location to minimize the chance of compression.
- Saphenous Nerve
- More-Vulnerable Locations: As it runs behind the inside of the knee.
- Rope Placement: Rope tied around the lower thigh near or behind the knee may cause compression.
- Results of Compression: Decreased sensation, numbness, tingling, or a burning sensation along the inner side of the lower leg and/or calf could indicate compression of the saphenous nerve.
- Peroneal Nerve
- More-Vulnerable Locations: As it runs from behind the knee and across to the outside of the knee.
- Rope Placement: Rope passing over the legs near the knee may cause compression as well as tight rope around the ankle.
- Results of Compression: Decreased sensation, numbness, tingling, or a burning sensation along the top of the foot, or the inability to flex the toes up towards the shin, could indicate compression to the peroneal nerve.
Sciatic Nerve: This nerve deserves mention here, though it would be extremely rare for it to be compressed by rope. Instead, this nerve is often affected by long periods of extreme flexion. For example, if the legs are held or tied back along the sides of the body for a long period of time (as in a position for sex), this may result in decreased sensation, numbness, tingling, or burning along the outside of the thigh and may also result in “buckling legs” … where the legs don’t seem to function correctly at first and need some time to recover before they feel stable again. (Also worth noting that those with pre-existing complications with their sciatic nerve will want to be particularly careful about the positions in which they are tied for any length of time.)
Innervation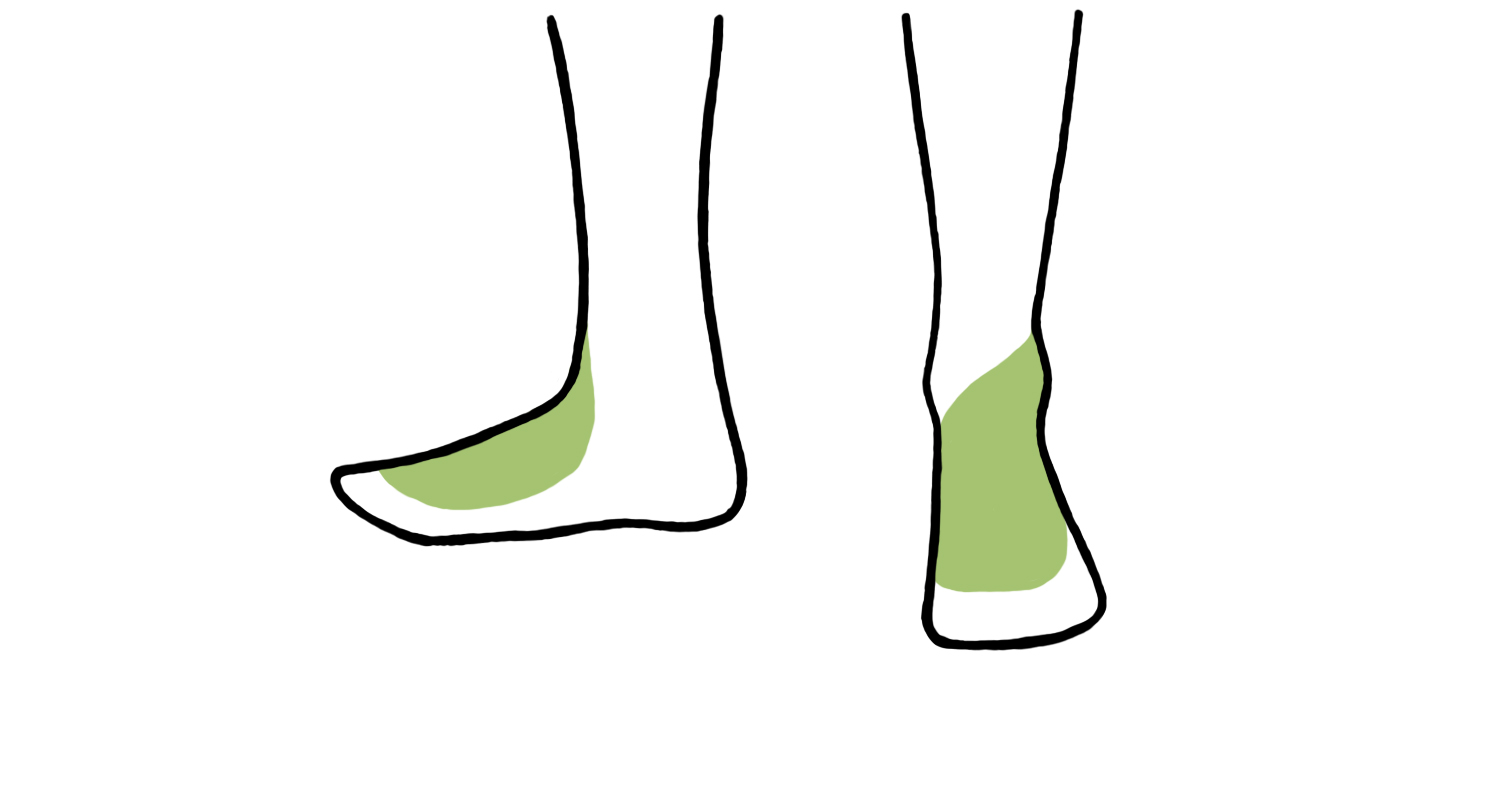
Mobility
Responding to Injury
PLEASE NOTE: Ultimately, it does not matter if you correctly identify which specific nerve is experiencing compression. Given individual variability and that nerve compression can happen at any point along the nerve and be caused by a variety of direct and indirect means, this can be difficult even for medical professionals. Do not waste time trying to determine which nerve is experiencing trauma. Instead, when sensation and mobility are compromised, respond immediately to alleviate all potential sources of compression and/or untie and follow the steps below.
At the first sign of potential nerve compression injury, take all necessary steps to relieve pressure in the affected area and/or possible sources of the compression. This may involve shifting the position to relieve pressure from the rope (which bottoms may also be able to do for themselves), but likely involves removing/untying the rope and/or ending the session completely and removing all rope.
The level of experience and risk profile of both the top and the bottom will determine your response. However, if changing position doesn’t cause immediate and noticeable relief, and untying in the specific area doesn’t cause immediate and noticeable relief, we advise ending the session and removing all rope. Please note that time is a significant factor in nerve compression injuries, and the sooner you address the issue, the more likely the issue will be minor and will heal quickly on its own. Every minute you delay can greatly increase the damage.
The current commonly-accepted initial treatment for nerve compression injuries is listed below. However, note that there are some disagreements in the medical community. We recommend reading “First aid for nerve damage” for a more complete understanding.
Assess Severity of the Injury
- If the injury involves sensation loss but no loss of mobility, and if the sensation returns within a few hours, there is likely no need to treat the injury beyond avoiding additional compression for a while to allow full healing.
- If the injury includes some loss of mobility, you should consider first-aid treatment as indicated below, monitor closely, and seek professional help if mobility does not improve within a 24-48 hours.
- In general, the more severe and/or longer lasting the symptoms, the more immediately you should seek professional help.
Response & Treatment
- As soon as indicators are detected, remove compression as soon as possible (in a controlled manner). It is typically best to avoid moving the body in any way that could cause “shearing forces” in the problem area. For example, don’t attempt to transition or rotate the bottom in rope before attempting to remove the pressure of the rope.
- Don’t stretch or massage the area and/or potential source location of injury. Your goal is to avoid any additional compression to the affected area until fully healed. (Remember that the actual site of the compression may not be in the area that is experiencing sensation or mobility issues.)
- Rest the area in the first few days of injury. (This may involve using a splint, depending on location and severity.)
- However, careful mobilization within the first week is also important. If the injury is significant enough to require more than a day or two to fully recover, physical therapy with a trained professional is recommended for finding the proper balance of rest, protection and mobility.
In all cases, and regardless of the first aid approach used: if symptoms do not lessen in 24-48 hours — or if there is pain and/or other symptoms accompanying the injury — see a doctor as soon as possible (with urgency determined by degree of mobility loss and/or pain).
Additional Information & Resources
Special thanks to RopeJester, Shayblondie, Hedwig, Topologist, MissDoctor, IPCookieMonster, Esinem, St3amPunk, and the many others who provided resources and suggestions, including the specific resources linked below.
Please spend time carefully reviewing these additional resources:
- The following videos by Topologist offer methods for both tops and bottoms to check for radial nerve compression. Also see his “Basic Safety” page for more information.
- We also recommend the video “Anatomy for Rope Bondage Safety,” which provides an excellent visual overview of the major areas of concern.
Remedial Ropes is an excellent resource for rope-bondage-related safety information.
- Please read the “Circulation” article
- Then read everything under the “Nerve Damage” section
- Then consider reading these additional articles from the site:
- “First Aid for Nerve Damage” (this is a longer version than the one in the section above)
- “On My Nerves”
- “It’s Just Decreased Circulation”
- “Once It’s Done It’s Done”
- “Six Contributing Factors to Nerve Damage in Bondage aka The Six Horsepeople of the Nervepocalypse“
- Other articles worth your time:
- “An Anthology for Nerve Compression Awareness“
- “Nerve Injury Education“
- “Rope – Nerve Damage Information”
- “Rope – Nerve Examination Tests”
- “Nerve and Circulation Problems”
- “Nerve Damage Study”
- “Nerve Injury Risk Awareness Information for the Rope Community”
- “Mobilization of the Plexus Brachialis Nerve Branch“
- “Bondage-relevant lessons learnt from ‘Going Out on a Limb’“
- “Tessin Doyama: On Kinbaku Safety“
- A cautionary tale: “Seven Months of Wrist Drop and Counting“
We also recommend the Zygote Body website to help you better visualize the location of various nerves in the body. There are other similar sites, but we’ve found this one to be particularly useful. Free accounts give you access to all the features you are likely to need.